Get the Best Treatment Options Based on Your Unique Diagnosis for the Little Rock Area, Central Arkansas, and Beyond
Skin cancer is a disease caused by the abnormal growth cells in skin tissue. It’s important to catch this type of cancer early as it can spread to surrounding tissues or other areas of the body if it is not treated. Whether a full-body skin exam at our office or a diagnosis elsewhere reveals skin cancer, Little Rock-area patients dealing with the common disease have options. The majority of skin cancers are cured when they are identified and treated in their early stages. Early detection of cancer gives you the highest chance of successfully treating this disease, so you should routinely check your skin for suspicious changes and have annual checkups with a dermatologist.
Contact Us Today
Schedule your consultation if you would like to discuss diagnosis and treatments for skin cancer for Little Rock, all of Central Arkansas, and beyond today. Call us at the Dermatology Group of Arkansas at 501-227-8422 or submit a contact form to request a consultation.

Skin Cancer Guide for 2025: What Causes Skin Cancer?
“What are the main causes of skin cancer?” is one of the most searched for dermatology-related questions online.
The normal skin cell turnover cycle involves cells growing old and dying, then being replaced with new ones. Cancer causes cells to grow more quickly, causing a malignant tumor to form. This tumor can potentially grow, causing damage to surrounding tissues. It can also metastasize, spreading cancer cells to other organs and systems in the body.
Skin cancer may have a genetic component, but in most cases, it is linked to both intense and cumulative exposure to UV (ultraviolet) rays from sunlight or from artificial sources such as tanning beds and sun lamps. Intense sunburns or blistering increase a person’s risk of developing the disease.
What Are the Different Types of Skin Cancer?
The skin is your body’s largest organ, and it consists of several layers, including the epidermis (the upper or outer layer of skin) and the dermis (the lower or inner layer). The epidermis contains three types of cells: squamous cells, basal cells, and melanocytes. Cutaneous cancer can develop in all three types of cells.
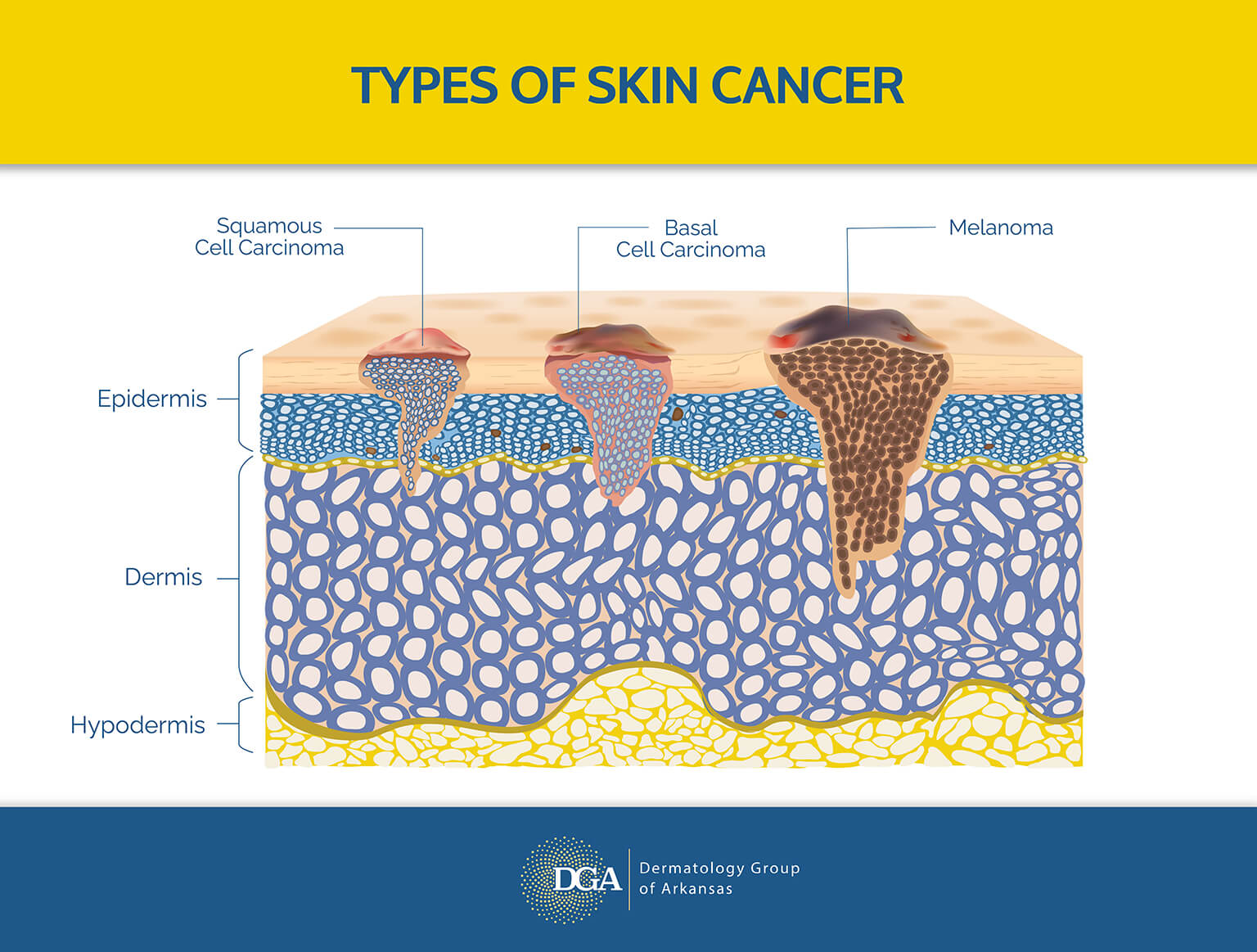
To find the most effective skin cancer treatment from the Little Rock area’s Dermatology Group of Arkansas, we will need to identify the type of skin cancer you have. This is determined by where the cancer originates. The three main types are basal cell carcinoma, squamous cell carcinoma, and melanoma. Basal cell carcinoma begins in your basal cells in the lower part of the epidermis while squamous cell carcinoma occurs in the squamous cells in the upper epidermis, and melanoma starts in the melanocytes – the cells that produce skin pigmentation.
What Are Basal Cell Carcinoma and Squamous Cell Carcinoma?
Basal cell carcinoma (BCC) is the most common type of skin cancer, accounting for about 80 percent of all skin cancers. Squamous cell carcinoma (SCC) is responsible for about 15 percent of all skin cancers. Both of these types of skin cancer are associated with sun exposure and a light complexion. Fortunately, both skin cancers can usually be treated successfully if identified early and handled appropriately.
BCC is a slow-growing skin cancer with very little ability to spread to other parts of the body. It can be locally invasive, however, growing into and destroying nearby structures such as the nose, ear, or eye. When located on the body, the skin cancer can grow large and invade down to muscle or bone and create an open wound, but this type of destruction usually takes several years to occur.
SCC is a more aggressive skin cancer than basal cell carcinoma skin cancer. It usually grows more quickly and can cause greater destruction than BCC skin cancer. In addition to being locally invasive, SCC can spread to lymph nodes or other parts of the body. This type of spread occurs most often in SCCs that are present on the lips, ears, hands, and fingers, as well as in patients whose immune systems do not work well. In the vast majority of cases, SCC remains only in the skin.
What Is Melanoma?
Melanoma is a potentially deadly skin cancer that comes from melanocytes, which are the cells in the skin that produce pigment. Fortunately, this type of cancer can usually be handled effectively if it is identified and treated in its early stages.
The prognosis for melanoma depends on the stage of the skin cancer at the time of diagnosis, which is based on specific features of the lesion and whether or not there is any evidence of this cancer elsewhere in the body.
The most important factor associated with survival in patients with melanoma is the thickness of the lesion. Thickness is most commonly reported as a measurement of depth given in millimeters, known as Breslow’s depth. Sometimes the thickness is reported in a different way— called the Clark’s level—which is designated with the Roman numerals I through V, with I being the thinnest and V being the thickest.
In general, the thicker melanoma is, the worse the prognosis. Some melanomas are designated as melanoma in situ, which means that the cancer is limited to the uppermost portion of the skin, dubbed the epidermis. Melanoma in situ has a long-term survival rate of nearly 100 percent when treated with appropriate skin cancer surgery.
Melanomas with a Breslow’s depth of less than 1 mm are considered thin melanomas and have a favorable long-term survival rate with appropriate surgical treatment. For skin cancers with a Breslow’s depth of greater than 1 mm, the long-term survival rate decreases as the depth increases.
For these thicker skin cancers, the lymph nodes are sometimes surgically removed and checked under a microscope for the presence of cancer cells. In these cases, whether or not cancer is detected in the lymph nodes becomes an important factor in predicting long term survival.
What Are the Signs and Symptoms of Skin Cancer?
Skin cancer often occurs on areas of the skin that are frequently exposed to the sun, but it can also occur on areas that do not normally get exposed to sunlight.
How can you tell if a spot is skin cancer? Lesions look different depending on the type you have.
A sudden change in your skin—such as a new growth or evolution in an existing mole—is a common sign of cancer. Some of the typical symptoms are a new mole, changes to the size, shape, and color of a mole, a pearly or waxy bump on the face or head area, or scar-like areas on the skin.
What Are the Risk Factors for Skin Cancer?
Although anyone can get skin cancer, there are certain groups that are more susceptible to the disease. Your risk will be higher if you spend a lot of time in the sun, get sunburned easily or have a history of sunburns, live in a sunny or high-altitude climate, have light-colored eyes, hair, and skin, have freckled skin, have a large number of moles or irregularly shaped moles, have a family history of skin cancer, or are taking medications that suppress or weaken your immune system.
Skin Cancer Prevention and Detection: What Can You Do to Reduce Your Risk of Skin Cancer?
Are there ways to prevent skin cancer? Regular sun protection can decrease your chances for developing future cancers. The following steps should be taken for sun protection. They are listed in order of importance, but should be used together whenever possible:
- Do not intentionally expose your skin to natural or artificial sunlight.
- Avoid sun exposure when possible, especially in the middle part of the day, when the sun is most directly overhead.
- Protect your skin from the sun with a physical barrier. Wear a hat with a broad brim, sunglasses, a long-sleeved shirt, and pants when outdoors.
- Apply a broad-spectrum sunscreen with an SPF of 30 or higher to all skin surfaces that you cannot cover with clothes.
A patient’s long-term outcome for skin cancer depends on a range of factors, including the stage at which the cancer is discovered. That’s why we recommend prevention first and foremost, as well as routine skin checks in order to spot and examine suspicious moles and lesions as early as possible.
What Should You Do If You Have Been Diagnosed with Skin Cancer?
What happens if you are diagnosed with skin cancer? What happens after a positive skin cancer biopsy? The first step is to get treatment for the skin cancer. After this is completed, you should schedule regular follow-up exams with your dermatologist, who will inspect the area where the skin cancer was treated to make sure the malignant cells are not growing back. The dermatologist will also check your skin for new skin cancers in other areas.
You should also examine your own skin thoroughly each month. Use a well-lighted room and the combination of a full-length mirror and a handheld mirror to check all of the areas that are hard to see. A spouse, parent, or friend can also help you. Notify us of any new growths, any spots that are changing, and any spots that “look funny.” Also pay attention to any spot that bleeds for no good reason or gets a scab that won’t heal. Most skin cancers are discovered by a patient or spouse and then brought to the attention of a doctor. Carefully examining your own skin is the best defense against a future skin cancer.
Once you have been diagnosed with BCC or SCC, you have a 50 percent chance of having another skin cancer within the next five years. Once you have been diagnosed with melanoma, you are in the highest risk group for developing a new melanoma. You should have a full skin exam by a dermatologist two to four times a year for the first five years after the melanoma has been diagnosed, and then at least once a year for the rest of your life.
If you have had melanoma, you need to let your primary care doctor know. You also need to let your doctor know if you develop any health changes, such as unintentional weight loss, severe headache, weakness, and jaundice. Other health care providers who should be notified of your history of melanoma include your dentist, your ophthalmologist, and your gynecologist.
You should notify all of your first-degree relatives—your parents, siblings, and children—that you have had a melanoma, as this skin cancer tends to run in families. All of your first-degree relatives should have a full skin exam by a dermatologist at least once a year.
Contact Us Today
Request your consultation if you would like to find out more about diagnosis and treatments for skin cancer for Little Rock, all of Central Arkansas, and beyond today. Call us at the Dermatology Group of Arkansas at 501-227-8422 or submit a contact form to schedule a consultation.
What Types of Treatments Are Available for Skin Cancer?
It can be scary to hear the words confirming what many people fear, but working with highly educated, trained, and experienced dermatologists— like the team at Dermatology Group of Arkansas—can make a difference.
The first step in treating BCC and SCC is to take a biopsy of the suspicious lesion to be checked under the microscope and make a definite diagnosis. Once this is done and cancer is confirmed, a skin cancer treatment can be chosen.
Several treatments are available for BCC and SCC, and each has its own specific advantages. Common treatments include destruction of the cancer and surgical removal of the cancer, either with Mohs surgery or traditional surgery. Less common treatments include radiation treatment and creams that can remove cancer. Sometimes multiple treatments are used in combination.
Your dermatologist at Dermatology Group of Arkansas will recommend the treatment he or she feels is most appropriate for you. If you have questions about treatments other than the one recommended, feel free to ask for more details.
Surgical removal is the main treatment for melanoma. The type of surgery recommended is determined by the depth of the melanoma. For melanomas with a Breslow’s depth of less than 1 mm, surgical removal of the melanoma with a margin of normal skin is needed.
This can usually be accomplished with an in-office skin cancer surgery performed with local anesthesia. It is not usually necessary to see another surgeon or to go to a hospital operating room. For melanomas with a Breslow’s depth of greater than 1 mm, it may be beneficial to have lymph nodes surgically removed in addition to the removal of the skin cancer. This surgery is usually performed in a hospital setting by a general surgeon or a cancer surgeon.
While surgery is the main treatment for melanoma and the skin cancer treatment with the greatest chance of a cure, some patients with melanoma have chemotherapy in addition to surgery. Chemotherapy is usually reserved for skin cancer patients whose melanoma has already spread to other parts of the body at the time of surgery or whose melanoma will likely spread in the future.
Meet Your Doctors




Meet Your Doctors


Meet Your Doctors







What Is a Sentinel Node Biopsy?
A sentinel lymph node biopsy is a type of surgery sometimes recommended for skin cancer patients with melanoma. The purpose of the surgery is to find out if melanoma has spread to the lymph nodes. A sentinel lymph node biopsy is usually performed in a hospital operating room and is done at the same time as the surgical removal of the melanoma.
Before the surgery, a radioactive dye is injected into the skin at the site of the cancer. Sensors are used to follow the path of the dye to the lymph nodes. This process identifies which lymph nodes are most likely to have melanoma if the skin cancer has spread there. Then your surgeon removes the melanoma and the lymph nodes identified by the dye. The lymph nodes are checked under the microscope for the presence of skin cancer cells.
Sentinel lymph node biopsy is not usually recommended for melanomas with a Breslow’s depth of less than 1 mm. If the Breslow’s depth of the skin cancer lesion is greater than 1 mm, a sentinel lymph node biopsy may be recommended.
Not all physicians agree about how important it is for skin cancer patients to have a sentinel lymph node biopsy performed, as the procedure has not been shown conclusively to increase the chances of curing melanoma. It does, however, provide valuable information for predicting how likely it is that the melanoma could result in death.
What Is Available Aside from Skin Cancer Treatments from the Dermatology Group of Arkansas?
Along with skin cancer diagnosis, care, and treatment, Dermatology Group of Arkansas also offers treatments for many other skin conditions such as psoriasis, rosacea, eczema, and actinic keratosis. We also provide cosmetic treatments to enhance the skin tone and appearance, such as BOTOX®, hyaluronic acid fillers such as Juvederm®, and biostimulatory injections like Sculptra®.

Contact Us Today
Contact the Dermatology Group of Arkansas today to learn more about identifying and treating skin cancer in the Little Rock area. Call 501-227-8422 or fill out a contact form to request a consultation.